
Where to Inject Peptides: Sites & Technique | PeptideIQ
Where to Inject Peptides: Complete Guide to Injection Sites & Technique
You have the vial. You have the syringe. Now you need to know exactly where to inject peptides — and how to do it without second-guessing every step.
Key Takeaways
- Subcutaneous (SQ) and intramuscular (IM) injections are the two primary delivery routes; SQ is the standard for most peptides due to ease and lower complication risk.
- Safe injection sites include the abdomen, outer thigh, upper arm, and glutes — rotating every injection prevents lipohypertrophy and maintains consistent absorption.
- Subcutaneous needles penetrate 0.5–1 inch at a 45–90° angle; IM needles go 1–1.5 inches at 90° into muscle tissue.
- Post-injection care and site inspection are essential — watch for warmth, redness, or swelling that persists beyond 24 hours.
- Understanding your specific peptide's delivery requirements before injecting ensures maximum bioavailability and protocol effectiveness.
Contents
- Where to Inject Peptides: What Are the Primary Sites?
- What Are the Best Injection Sites for Peptides?
- What's the Difference Between Subcutaneous and Intramuscular Peptide Injections?
- How Deep Should a Peptide Injection Go?
- Does It Matter Where to Inject Peptides, or Can You Use SQ for All of Them?
- How Often Should I Rotate My Peptide Injection Sites?
- What Should I Do If I Hit a Blood Vessel During a Peptide Injection?
- Why Is Injection Site Rotation Critical for Peptide Therapy?
- Why PeptideIQ's Injection Guide Matters for Your Protocol
- Frequently Asked Questions
Where to Inject Peptides: What Are the Primary Sites?
The four primary sites for peptide injections are the abdomen, outer thigh, upper outer arm, and upper glutes. For subcutaneous administration — which covers the vast majority of peptides — the abdomen is the most commonly recommended site due to consistent tissue depth, easy access, and predictable absorption rates.
Most users default to the abdomen because it offers the largest surface area and is the most forgiving for beginners. Each site has practical trade-offs worth knowing before you commit to a routine.
 The four primary peptide injection zones — each with distinct tissue depth and absorption characteristics.
The four primary peptide injection zones — each with distinct tissue depth and absorption characteristics.
Key insight: No single site is universally "best" — the right site depends on your peptide type, your body composition, and how easily you can self-administer.
What Are the Best Injection Sites for Peptides?
The best peptide injection sites balance tissue accessibility, consistent absorption, and rotation capacity. The abdomen offers the most flexibility; the outer thigh is ideal for self-injection of IM peptides; the upper arm and glute work well for those with assistance or advanced technique.
Here's how each site compares:
Abdomen
The most popular site for subcutaneous peptide injections. Inject at least 2 inches away from the navel — tissue near the belly button is too fibrous for clean absorption. The abdomen provides 8–10 distinct rotation zones and maintains consistent tissue depth across most body types.
Outer Thigh
The front-outer quadrant of your thigh — roughly one hand-width above the knee to one hand-width below the hip crease. This is the go-to IM site for self-administration since you can stabilize your leg and inject without contorting.
For subcutaneous thigh injections, pinch a fold of skin on the outer surface. Avoid the inner thigh — it has more vascularity and is prone to bruising.
Upper Outer Arm
The fatty tissue over the deltoid — harder to self-administer due to the angle required, more practical when someone else injects for you. For IM injections, the deltoid handles volumes under 1 ml; the vastus lateralis (outer thigh muscle) is better for larger volumes.
Upper Glutes
The upper-outer quadrant of each buttock — about two finger-widths below the hip bone and lateral from the gluteal fold. A common IM site for larger-volume injections. Self-administration requires practice; most beginners start with abdomen or thigh.
What's the Difference Between Subcutaneous and Intramuscular Peptide Injections?
Subcutaneous (SQ) injections deposit peptides into the fat layer just beneath the skin, where they absorb slowly and steadily. Intramuscular (IM) injections go deeper into muscle tissue for faster uptake. Most peptides — including BPC-157, GLP-1s, GHK-Cu, and GHRPs — use the subcutaneous route by default.
The choice between SQ and IM isn't about preference — it's dictated by the peptide's pharmacokinetics and manufacturer guidance.
| Feature | Subcutaneous (SQ) | Intramuscular (IM) |
|---|---|---|
| Needle depth | 0.5–1 inch | 1–1.5 inches |
| Injection angle | 45–90° | 90° |
| Absorption speed | Slower, sustained | Faster |
| Pain level | Minimal | Mild to moderate |
| Common peptides | BPC-157, GLP-1s, GHK-Cu, GHRPs | TB-500 (some protocols), larger-volume compounds |
| Preferred sites | Abdomen, outer thigh | Vastus lateralis, deltoid, glute |
| Beginner-friendly | Yes | Moderate difficulty |
Bottom line: If your protocol doesn't specify IM, assume SQ. The vast majority of self-administered peptides use subcutaneous delivery.
How Deep Should a Peptide Injection Go?
For subcutaneous peptide injections, the needle should penetrate the skin 0.5 to 1 inch, entering the fatty layer beneath. For intramuscular injections, the target depth is 1 to 1.5 inches into muscle tissue. Using the wrong depth is one of the most common beginner errors — injecting too shallow leaves the peptide in the dermal layer; too deep risks hitting muscle or vasculature unintentionally.
The correct depth also depends on body composition. A leaner person may need a shallower angle; someone with more subcutaneous fat can inject at a steeper angle and still land in the right layer.
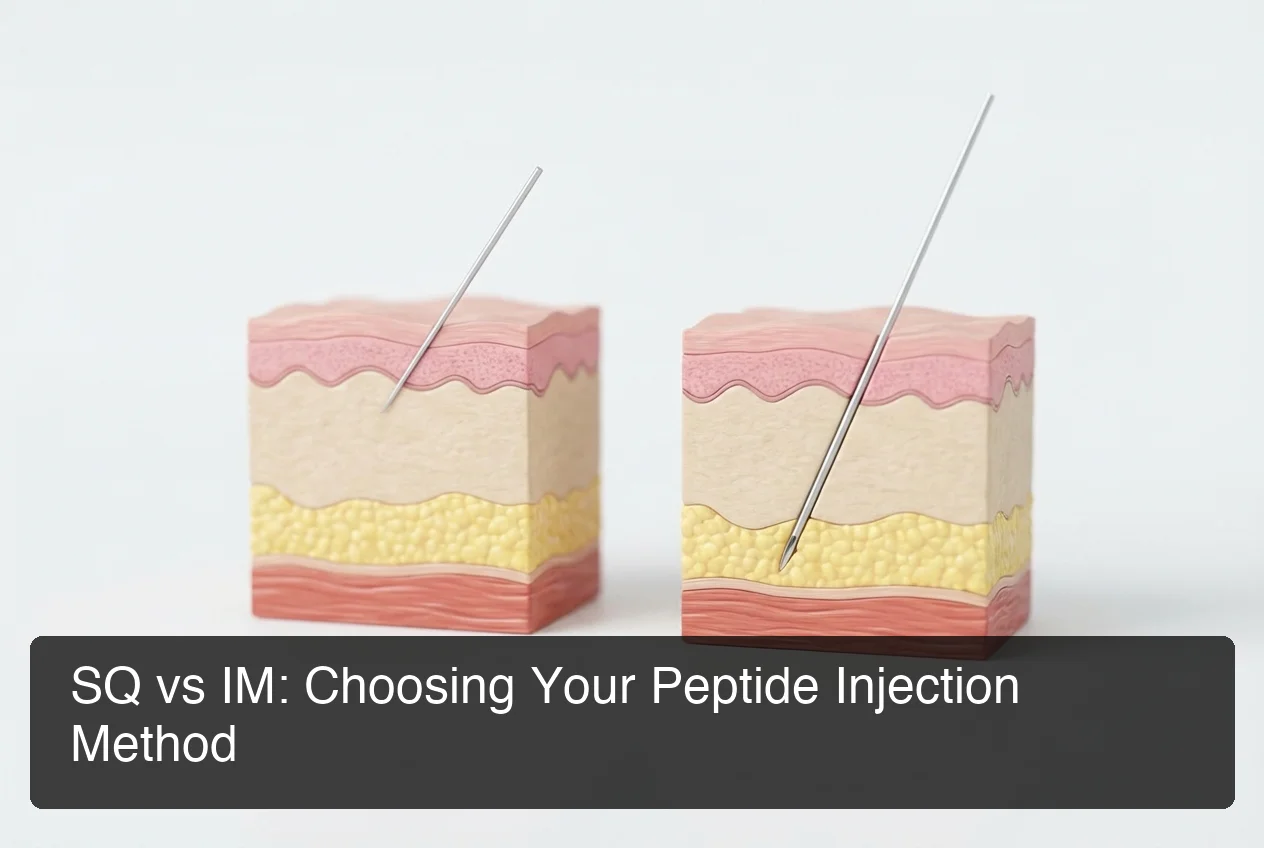
 Proper needle angle and tissue layering — depth matters as much as site selection.
Proper needle angle and tissue layering — depth matters as much as site selection.
Needle Angles Explained
- 45° angle: Standard for most SQ injections, especially in areas with thinner fat layers like the upper arm and thigh.
- 90° angle with pinched skin: Ideal for the abdomen — pinch a fold to lift the fat layer away from muscle. Standard for GLP-1 protocols.
- 90° angle without pinch: Used for intramuscular injections where full muscle penetration is intended.
Most subcutaneous peptide injections use insulin syringes — 28–31 gauge, 0.5–1 inch needles. For peptides, always use the highest gauge number (thinnest needle) your peptide's viscosity allows. A 31G x 5/16" needle is the most common choice.
By the numbers: Pain from subcutaneous peptide injections should be minimal — most discomfort traces back to injection angle errors or cold solution, not the needle itself.
Does It Matter Where to Inject Peptides, or Can You Use SQ for All of Them?
Most peptides — BPC-157, semaglutide, tirzepatide, GHK-Cu, Ipamorelin, CJC-1295, and most GHRPs — are formulated for subcutaneous administration. A smaller subset, including some TB-500 protocols and certain growth hormone formulations, may specify intramuscular or even intranasal routes. Always follow the specific peptide's established protocol, not a generic injection guide.
Like all peptide users, those managing Ozempic or semaglutide protocols must understand proper injection technique to minimize side effects — the same injection-site principles apply across the GLP-1 family.
Before committing to any injection protocol, it's worth checking the regulatory status of your specific compound — our list of FDA-approved peptides covers which compounds have cleared the approval threshold and which remain in gray-market territory.
Peptides by Preferred Route
| Peptide | Preferred Route | Notes |
|---|---|---|
| BPC-157 | SQ or IM | SQ near injury site for local effect; systemic SQ for general use |
| Semaglutide / Tirzepatide | SQ | Always subcutaneous — abdomen, thigh, or upper arm |
| Ipamorelin / CJC-1295 | SQ | Fasted administration required |
| GHK-Cu | SQ | Topical alternatives exist for skin-focused use |
| TB-500 | SQ or IM | Some protocols prefer IM for faster systemic uptake |
| Sermorelin | SQ | Subcutaneous only; bedtime dosing common |
| GHRP-2 / GHRP-6 | SQ | Fasted, multiple daily doses typical |
How Often Should I Rotate My Peptide Injection Sites?
Rotate your peptide injection site every single injection. Never inject the same point twice in a row. The minimum rotation cycle should cover 4–8 distinct sites before returning to any one location. Most experienced users maintain a systematic rotation across the abdomen (left, right, upper, lower quadrants) and alternate with thigh or arm sites.
A structured rotation protocol looks like this:
- Left abdomen (upper)
- Right abdomen (upper)
- Left abdomen (lower)
- Right abdomen (lower)
- Left outer thigh
- Right outer thigh
- Back to left abdomen (upper) — at least 48 hours have passed
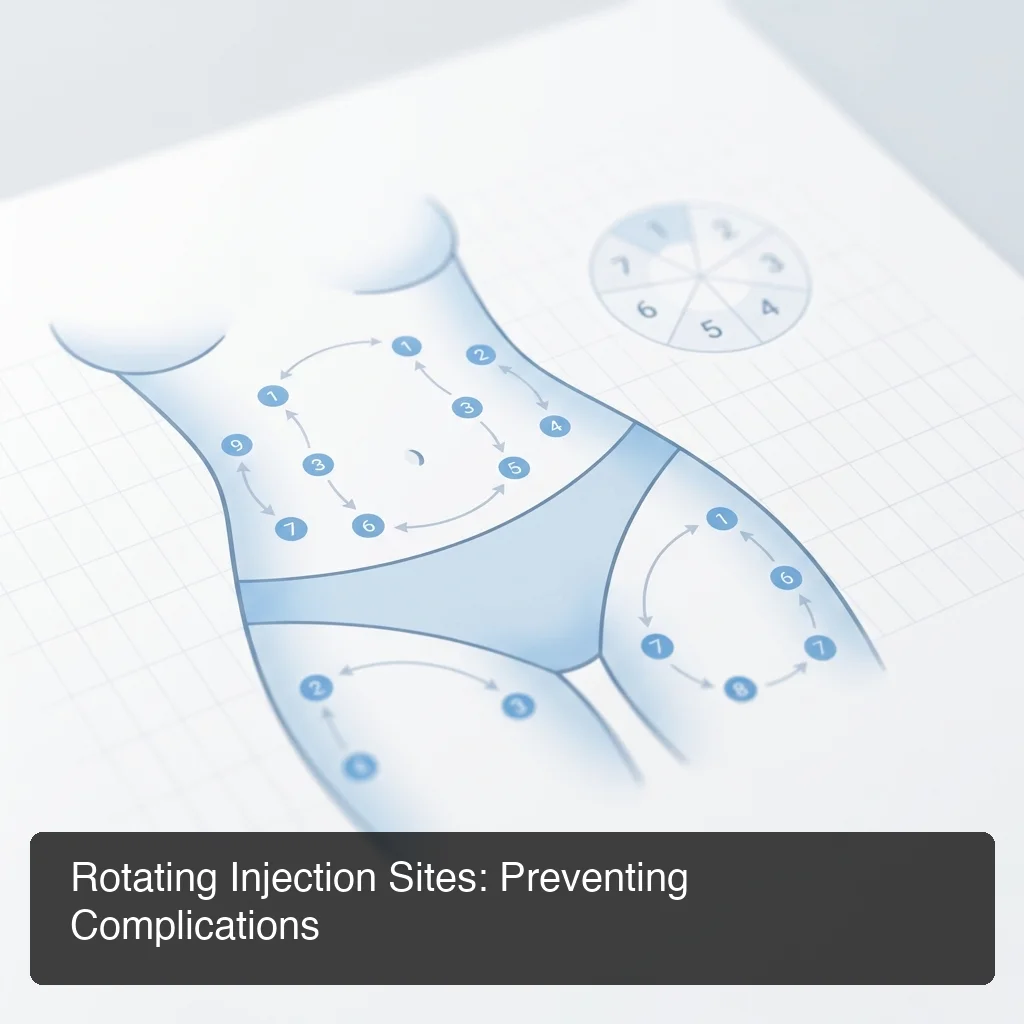 A systematic rotation grid prevents lipohypertrophy and maintains consistent peptide absorption.
A systematic rotation grid prevents lipohypertrophy and maintains consistent peptide absorption.
Key insight: Rotation isn't optional — it's the difference between a protocol that works consistently for 8 weeks and one that develops absorption problems at week 4.
For daily injectors (common with GHRPs, BPC-157, and most GLP-1 protocols), you're moving through your rotation sites constantly. Map them out before day one.
What Should I Do If I Hit a Blood Vessel During a Peptide Injection?
If blood appears in the syringe barrel when you aspirate (or draw back the plunger slightly), withdraw the needle immediately, apply gentle pressure with a clean gauze or cotton ball, and choose a new injection site. Do not inject the dose into a blood vessel — IV administration of peptides intended for subcutaneous delivery bypasses the intended release mechanism and increases risk of adverse reactions.
Step-by-step response: stop immediately, withdraw the needle smoothly, apply light pressure with clean gauze for 1–2 minutes, discard the syringe, draw a fresh dose, and choose a new site at least 2 inches away.
Most users never hit a vessel with proper subcutaneous technique. The risk is higher at the inner thigh and upper arm. Using a 45° angle and staying on the outer surfaces dramatically reduces this risk.
Why Is Injection Site Rotation Critical for Peptide Therapy?
Site rotation prevents lipohypertrophy — the buildup of scar tissue and fatty deposits at repeatedly injected sites. Lipohypertrophy doesn't just feel like a lump; it actively impairs peptide absorption, creating an unreliable delivery zone that reduces the effective dose reaching systemic circulation. This directly undermines your protocol's results.
Insulin therapy research established this clearly: repeated injections at the same site cause tissue damage, scar formation, and reduced vascularity. Absorption rates drop an estimated 20–40% in lipoatrophied tissue compared to healthy sites.
Signs You've Over-Used a Site
- A firm or rubbery lump under the skin
- Reduced sensation in the area compared to surrounding tissue
- Reduced stinging or pressure during injection (paradoxically — scar tissue has fewer nerve endings)
- Visible indentation or discoloration over time
If you identify a developing site problem, rest it completely for 4–6 weeks. Rotate to your other zones. The tissue often partially recovers.
Improper injection also carries infection risk beyond lipohypertrophy — for a full picture of what can go wrong and how to mitigate it, see our guide on peptide safety considerations.
Bottom line: Consistent rotation isn't just good practice — it directly determines whether your protocol delivers the dose you calculated. Scar tissue is invisible until the results stop coming.
Why PeptideIQ's Injection Guide Matters for Your Protocol
 Understanding injection depth is foundational — and it's only one piece of a complete protocol system.
Understanding injection depth is foundational — and it's only one piece of a complete protocol system.
Knowing where to inject peptides is table stakes. Executing it correctly, consistently, across a multi-week cycle — while tracking dose timing, site rotation history, and biomarker responses — is where most self-managed protocols break down. Once you have the sites and angles down, the next step is mastering how to inject peptides with the correct prep and technique sequence.
PeptideIQ is the guided AI system built for exactly this problem. The app includes a visual injection site rotation tracker with a front-and-back body diagram — green for ready sites, yellow for recently used, red for today's injection. It recommends the next site automatically based on your rotation history and tells first-timers the exact anatomical landmark: "Left abdomen — 2 inches from navel."
Join the PeptideIQ waitlist at peptideiq.io
Not starting a protocol yet? Join the waitlist for early access and our complete peptide beginner's guide — free when we launch.
Frequently Asked Questions
Where is the best spot to inject peptides?
The abdomen is the most recommended site for most peptide users because it offers large surface area for rotation, consistent subcutaneous tissue depth, and easy self-access. The outer thigh is the best secondary site. Both should be rotated systematically every injection to prevent lipohypertrophy and maintain absorption.
Do you inject peptides in fat or muscle?
Most peptides are injected subcutaneously — into the fat layer just beneath the skin, not into muscle. Subcutaneous injection creates a slow, sustained absorption curve suited to peptide pharmacokinetics. Intramuscular injection (into muscle) is specified for a smaller subset of peptides requiring faster systemic uptake.
How do I know if I'm injecting subcutaneously vs. intramuscularly?
For subcutaneous injection: pinch a fold of skin and insert the needle at 45°, entering the fatty tissue beneath. For intramuscular injection: no pinch, 90° angle, needle goes 1–1.5 inches into the muscle belly. If you feel significant resistance or the injection area aches deeply afterward, you may have gone intramuscular unintentionally.
Can I inject peptides anywhere on my body?
No — injection sites are limited to areas with adequate subcutaneous fat or accessible muscle tissue: abdomen, outer thigh, upper outer arm, and upper glutes. Avoid the inner thigh (vascular risk), directly over joints, areas with active skin conditions, and within 2 inches of the navel for abdominal injections.
How do I prevent lumps at injection sites?
Rotate sites every injection across a minimum 4–8 point rotation grid, use the correct needle gauge and angle, inject slowly, and warm the injection site gently before injecting. Let refrigerated peptides reach room temperature before injecting — cold solutions cause more tissue irritation and localized inflammation.
What needle size should I use for peptide injections?
For subcutaneous peptide injections, a 28–31 gauge, 0.5-inch insulin syringe is standard. The 31G x 5/16" is the most common choice — it's short enough to prevent accidental IM penetration in lean areas and thin enough to minimize injection pain. Intramuscular injections typically require a 23–25G, 1–1.5 inch needle.
Is it safe to inject peptides without medical supervision?
Safety depends on the peptide type, dose, and source quality. FDA-approved peptides (semaglutide, tirzepatide) are typically obtained through prescription with some clinical oversight. Gray-market peptides (BPC-157, GHK-Cu, GHRPs) carry higher risk due to variable product quality and no prescriber guidance. Learning proper injection technique and monitoring your response systematically reduces risk significantly in either case.